



Evidence from a randomised evaluation in Mexico shows that an AI-powered mental health app can improve mental health, daily functioning, and labour market outcomes, while also helping users experiencing more severe psychological distress engage with formal care.
Mental health disorders are a major cause of disability worldwide, but access to care remains severely limited (Patel et al. 2018). The scarcity of trained providers, cost of treatment, stigma, and practical difficulties of accessing care prevent many people from seeking help. The ubiquity of smartphones has created new opportunities to offer digital care at scale. AI-powered wellbeing apps in particular can provide personalised, on-demand mental health and wellbeing support at low cost.
Scalable but new technology
Existing research has shown that structured psychological interventions delivered through schools, communities, and lay providers can improve mental health outcomes in low-resource settings (Angelucci et al. 2026, Patel et al. 2017, Edmonds et al. 2025). Many of these interventions draw on principles of cognitive-behavioural therapy (CBT), which helps individuals develop coping strategies, reframe negative thought patterns, and build healthier behavioural routines.
AI-powered tools based on CBT principles may offer another avenue for scaling personalised, on-demand mental health support at low cost, allowing individuals to access help in a flexible, discreet, and affordable way. AI systems can adapt interactions dynamically, responding to users’ emotional states and guiding them towards exercises or coping strategies tailored to their needs.
Despite this potential, questions remain about both the impacts of and demand for this technology. Use of digital mental health products often declines rapidly over time (Baumel et al. 2019), raising concerns that users may disengage before benefits materialise. There are also concerns that these tools may be ineffective, exacerbate feelings of isolation, or generate other unintended negative effects.
Evidence on AI-powered digital apps
In recent work, we studied the impacts of offering an AI-powered mental health app to women in Mexico experiencing psychological distress (Angelucci, Fabregas, and Vazquez 2026). We partnered with a Mexican company to evaluate Mindsurf, a wellbeing app which draws on principles of CBT to provide features commonly used in evidence-based psychological interventions, such as mood tracking, guided audio exercises, self-assessment tools, and an AI-powered conversational agent that provides support and guidance. The AI assistant was designed as a restricted conversational agent, limited to CBT-informed topics and intended to guide users towards structured activities such as behavioural activation. The app also incorporates multiple safety features and guardrails.
We recruited 1,964 women in Mexico experiencing at least mild psychological distress and randomly assigned half to receive access to the app for up to six months. We then collected data on mental health and socioeconomic outcomes at 1, 2, and 6 months, as well as weekly wellbeing measures from all participants. We also obtained administrative data on app engagement.
Persistent wellbeing and behavioural improvements despite declining engagement
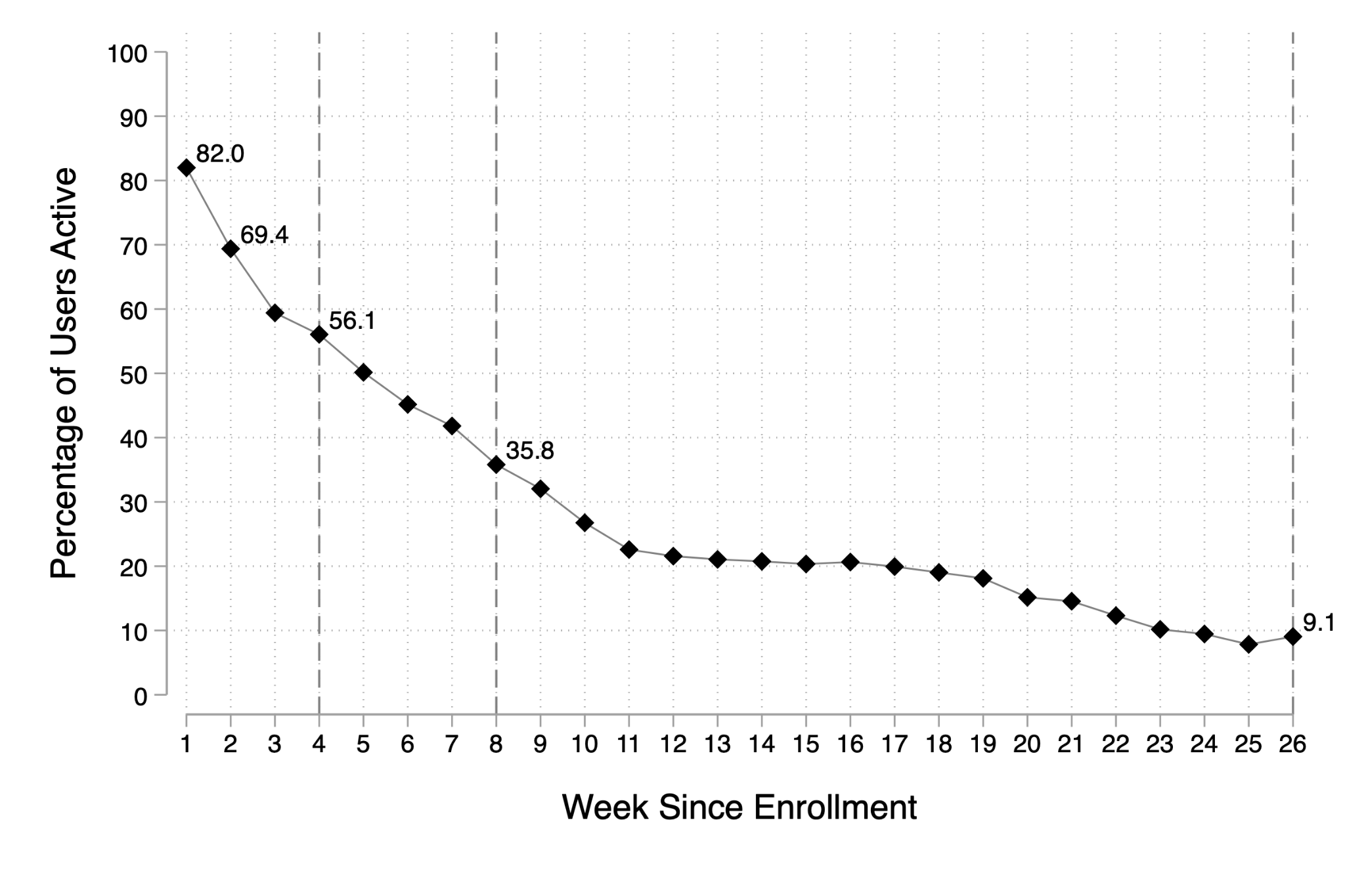
Figure 1: Engagement with the app over time and weekly measures of positive affect
a) Weekly active app use
b) Weekly treatment effects on positive affect
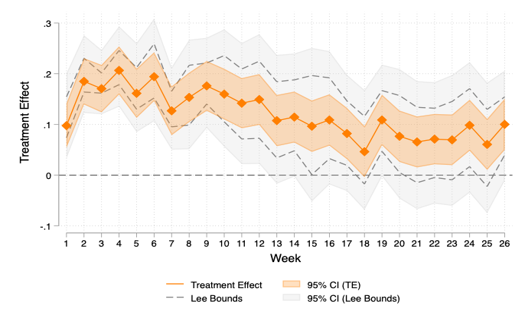
Notes: Panel (a) shows the share of treatment-group participants actively using the app in each week following enrolment. Panel (b) reports weekly intention-to-treat (ITT) coefficients from regressions of an indicator for reporting feeling happy on treatment assignment. Error bars represent 95% confidence intervals. Lee (2009) bounds are shown in lighter shading.
App use in the treatment group started high but declined substantially over time: from 82% at week 1 to 36% and 9% at 8 and 26 weeks, respectively (Figure 1, Panel a). This rapid decline is common among digital products. Nevertheless, positive effects emerged quickly. Those in the treatment group reported higher levels of positive affect as early as the first week after enrolment (Figure 1, Panel b). Over the first six months, access to the app reduced the prevalence of moderate-or-higher depression and anxiety symptoms by 12.6 and 8.7 percentage points, respectively, a 20% reduction relative to the control group for both outcomes (Figure 2).
Figure 2: Effects of access to the app on depression and anxiety symptoms
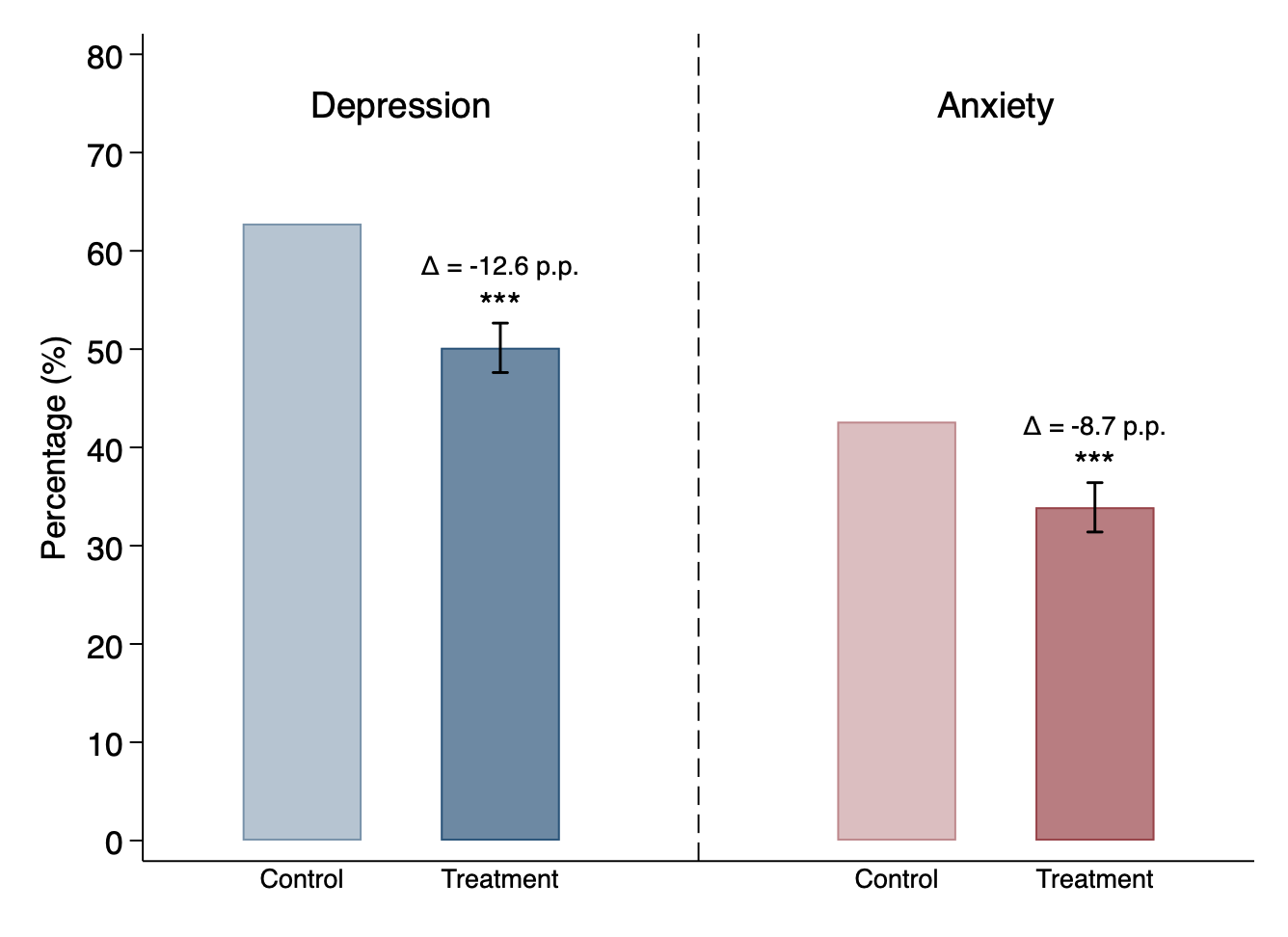
Notes: The figure reports pooled ITT estimates across three survey waves. Outcomes are indicators for moderate-or-higher depression symptoms (PHQ-8 score ≥ 10) and moderate-or-higher anxiety symptoms (GAD-7 score ≥ 10). Bars show group means in the control and treatment groups.
Across a broader mental health index combining multiple measures of wellbeing and psychological distress, we find improvements of approximately 0.3 standard deviations. These effect sizes are comparable to those reported for first-line treatments such as antidepressants and scalable lay-delivered talk therapy (Gartlehner et al. 2017, Singla et al. 2017, Cuijpers et al. 2023).
Participants also reported improvements across a broader set of wellness and functioning behaviours. Among our prespecified outcomes, we find that participants gained approximately 10 minutes per night in sleep, 0.3 days per week going out, a 10% reduction in high social media use (defined as at least two hours per day), and two fewer days of missed work over a six-month period (Figure 3).
Figure 3: Effects of access to the app on selected wellness and functioning behaviours
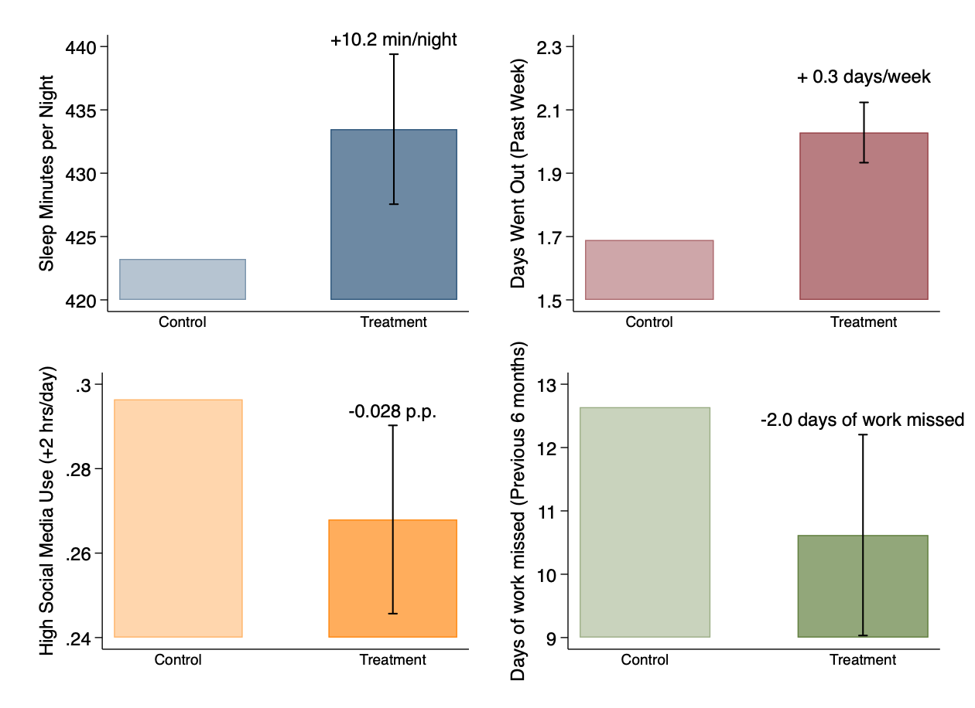
Notes: The figure reports pooled ITT estimates across three survey waves. Outcomes are average minutes of sleep per night, days went out in the past week, an indicator for high social media use (more than two hours per day), and days of work missed in the previous six months. Bars show group means in the control and treatment groups.
The persistence of mental health and behavioural improvements despite declining engagement suggests that participants may have internalised tools and behavioural strategies from the app and continued to apply them outside the platform, even after active usage fell. We find suggestive supporting evidence for this interpretation.
AI as a gateway to care?
The app increased, rather than reduced, the use of psychotherapy. These effects were concentrated among women with higher levels of baseline psychological distress, a group with both greater need for care and potentially larger barriers to accessing it. We find suggestive evidence that the app may have helped reduce non-monetary barriers to seeking treatment among these women.
This pattern challenges concerns that AI will replace therapists. Instead, our findings suggest that this technology may sometimes complement in-person care, for example, by helping high-need individuals take steps towards seeking treatment from a mental health professional.
Implications for mental health policy
The rapid growth of AI has generated both excitement and scepticism across many sectors, including mental health care. Our work shows that AI-enabled digital mental health tools can generate considerable improvements in wellbeing at relatively low cost. Moreover, these tools may help high-need individuals access formal care by lowering non-monetary barriers to treatment.
The persistence of mental health and behavioural improvements despite declining app use also has important implications for how digital interventions are evaluated. Many assessments of digital products focus heavily on engagement metrics such as active users, time spent on a platform, or retention rates. Our findings suggest caution in relying on these measures alone. For some interventions, benefits may persist even after active use declines, meaning that engagement and impact can become decoupled over time. More broadly, this may also have implications for how digital mental health tools are financed and delivered. If benefits persist after users reduce or discontinue active use, consumers may stop paying for ongoing access even as they continue to benefit. Under subscription-based business models, which charge for continued access rather than realised benefits, firms may be unable to capture the full social value they create, leading to a socially inefficient underprovision of this class of products.
Digital mental health care alone will not close the global mental health treatment gap. However, it has the potential to be a cheap, scalable and effective tool to address the unmet global mental health care needs, particularly in low-resource settings.
References
Angelucci, M, D Bennett, R Fabregas, and A Vazquez (2026), "Mental health and investment propensity: Evidence from India and Mexico," Unpublished manuscript.
Angelucci, M, R Fabregas, and A Vazquez (2026), "The well-being effects of digital mental health care," Unpublished manuscript.
Baumel, A, F Muench, S Edan, and J M Kane (2019), "Objective user engagement with mental health apps: Systematic search and panel-based usage analysis," Journal of Medical Internet Research, 21(9): e14567.
Cuijpers, P, C Miguel, A Ciharova, et al. (2023), "The effects of psychotherapies for depression on response, remission, reliable change, and deterioration: A meta-analysis," World Psychiatry, 22(1): 105–115.
Gartlehner, G, R A Wagner, K Matyas, et al. (2017), "Pharmacological and nonpharmacological treatments for major depressive disorder: Review of systematic reviews," BMJ Open, 7(6): e014912.
Edmonds, E, P Mukherjee, N Prakash, N Prakash, and S Sabarwal (2025), "Talk therapy and human capital in adolescence: Evidence from a low-resource setting," Unpublished manuscript.
Lee, D S (2009), "Training, wages, and sample selection: Estimating sharp bounds on treatment effects," Review of Economic Studies, 76(3): 1071–1102.
Patel, V, S Saxena, C Lund, G Thornicroft, F Baingana, P Bolton, D Chisholm, P Y Collins, J L Cooper, J Eaton, et al. (2018), "The Lancet Commission on global mental health and sustainable development," The Lancet, 392(10157): 1553–1598.
Patel, V, B Weobong, H A Weiss, A Anand, B Bhat, B Katti, S Dimidjian, R Araya, S D Hollon, M King, L Vijayakumar, et al. (2017), "The Healthy Activity Program (HAP), a lay counsellor-delivered brief psychological treatment for severe depression, in primary care in India: A randomised controlled trial," The Lancet, 389(10065): 176–185.
Singla, D R, S Kohrt, J Murray, A Anand, and V Patel (2017), "Psychological treatments for the world: Lessons from low- and middle-income countries," Annual Review of Clinical Psychology, 13: 149–181.